Insights
4 August 2015
Drug Safety: which compounds are at risk of adverse cognitive effects?
What compounds are likely to impair cognition and how to know if a compound could affect cognitive function.
How do I know if my compound could affect cognitive function?
Cognition is essential for the intake, interpretation and storage of information about the world around us and how we then use that information to interact with our environment. There are many things that can affect our perception, understanding and decision making processes whilst carrying out everyday activities. For example, neurological conditions and psychiatric disorders, such as Alzheimer’s disease or schizophrenia, are well-known to be linked with cognitive problems and often cognitive impairment is considered a primary characteristic of the disorder. In addition, the ageing process itself is associated with a natural deterioration of certain cognitive functions, such as memory.
It is becoming increasingly accepted that side-effects of medication could include cognitive impairment (e.g. confusion, memory loss) and self-reports of perceived cognitive problems, such as memory loss, by patients is becoming more and more frequent. It is therefore important that clinical development programs for compounds that are known to affect function of the central nervous system (CNS) include assessments of cognitive safety in order that a drug’s cognitive profile can be characterized early on in the development process, rather than via consumers post-marketing.
So, which compounds can affect CNS function?
Compounds that penetrate the CNS
Generally speaking, any small molecule that can cross the blood brain barrier has the potential to affect the CNS and therefore alter cognitive functioning. Agents that modulate the brain’s neurotransmitter systems (e.g. dopamine, glutamate, serotonin and acetylcholine) could either enhance or impair particular cognitive functions. This can be demonstrated by an inverted-U function where the optimal dose of a drug results in improvement of cognition, whilst other doses can cause cognitive impairments (see Figure 1). It is worth noting that cognitive enhancing drugs developed for a specific disease, at acute or high doses, may impair cognition in healthy individuals (e.g. donepezil; a drug developed for Alzheimer’s type dementia) and supports the need to conduct dose-escalation studies in early phase development.

Figure 1. Example of an inverted-U function.
In addition to brain modulators, blockers of neurotransmitter receptors can also result in cognitive impairment and includes compounds such as dopaminergic, cholinergic and histaminergic antagonists. Finally, drugs that are known to alter mood or anxiety and sedative properties of certain drug classes (e.g. antihistamines, hypnotics) also suggest opportunities for cognitive impairment to occur.
Non-CNS compounds that indirectly affect CNS function
Whilst it is well-established that clinical treatments for CNS disorders have a risk of impairing cognition, it is less well-known that compounds developed for non-CNS disorders also have the potential to impact cognitive function. Known examples include treatments for cardiovascular disease (i.e. statins), allergies (i.e. antihistamines) and oncology (i.e. chemotherapy). These compounds have the potential to indirectly affect the CNS and the process by which cognition is affected is not always clear. In addition, drugs intended to modulate the heart, affect breathing, the immune system or glucose transport use mechanisms that communicate with the CNS in one way or another and therefore increase the possibility of an associated impact on cognitive function.
Drug-drug interactions
It is not uncommon today for individuals to be taking multiple medications on a regular basis, particularly those who suffer from several co-morbidities such as hypertension, diabetes and cardiovascular disease. Individuals over 65 are the largest consumers of prescription and non-prescription medications in the US and 29.4% of them are prescribed 6 or more concurrent drugs1. Drug-drug interactions can have synergistic effects on cognition. For example, a study showed that benzodiazepine and an antipsychotic, when taken independently by healthy volunteers, had no significant effect on reaction times. However, when the medications were administered concurrently, deleterious effects on reaction times were observed equivalent to that of when someone is over the drink-driving limit2 (see Figure 2). Individuals who suffer from co-morbidities are typically excluded from clinical development trials and therefore unanticipated drug effects on cognition such as these are often only uncovered post-approval.
Example of drug-drug interactions and the impact on cognition
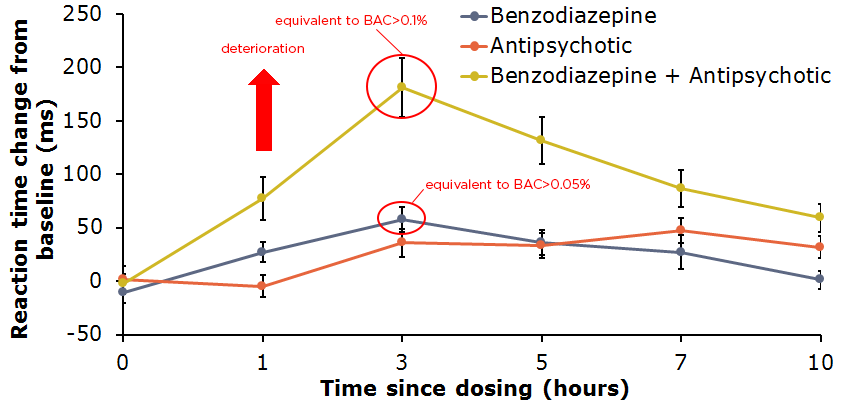
Figure 2. Effect of benzodiazepine and an antipsychotic on reaction time when taken independently and concurrently. BAC = blood alcohol level.Improving outcomes throughout clinical development
All drug compounds have the potential to impair cognition, it is important for clinical trials to further investigate the cognitive effects of treatments both for CNS and Non-CNS disorders, as well as, thinking about drug-drug interactions. Clinical trials would benefit from cognitive safety and efficacy assessments throughout all stages of clinical development. Cambridge Cognition has experience in supporting pharmaceutical and biotech companies improve outcomes in clinical studies with CANTAB cognitive assessments for over 30 years.
Find out more about using CANTAB in drug development.
Watch Dr Kenton Zavitz’s speech on cognitive safety assessments at the World Drug Safety Congress
References
1 Bushardt, R.L., Massey, E.B., Simpson, T.W., Ariail, J.C. & Simpson, K.N. (2008), Polypharmacy: Misleading, but manageable, Journal of Clinical Interventions in Aging, 3(2), 383-389.
2 Internal Cambridge Cognition data
